Kuldeep Singh Rajput is currently a PhD research scholar at National University of Singapore (NUS). He participated in a series of camps (REDX and Kumbhathon) partly organized by Camera Culture group. The resultant project, mECG, has won many awards, has been deployed and the team is exploring a commercial venture with govt and private funding. Kuldeep shares his fascinating journey from getting noticed for his final year bachelors project to REDX camps and beyond. He is returning to REDX and Kumbathon as an instructor in January 2015.
I first felt the thrill of becoming a scientific researcher when I presented a project at the Indian National Children’s Science Congress. I was 16 and I was given the Junior Scientist award. Now, as an adult, my passion continues to push me to excel and innovate.
I’m presently a PhD Research Scholar at National University of Singapore. My research mainly focuses on neuro-devices, massive neural stimulation, recording and data analysis. As a part of TSS Group I have started working on designing a1024 channel Optical Stimulator for In-Vitro Neuroscience experiments.
I first met Professor Ramesh Raskar, during my senior year of undergrad where I showed him the Brain Controlled Wheelchair which was part of my undergrad thesis. He was impressed by this invention for the paralyzed. Before he left, he handed me his visiting card said, “You are doing cool stuff! Stay in touch.”
One fine day, I received an email from Ramesh asking me to join the ReDx: MIT Health Tech Workshop in Mumbai. ReDx stands for Rethinking Engineering Design Execution. I immediately agreed, very excited about the opportunity. In this workshop, I started working with Rohan Puri and Dr. Maulik Majmudar on designing a low-cost, wearable, continuous ECG monitoring device with automated diagnosis for various cardiovascular diseases. Our team ‘mECG’ consisted of some amazing people having wide range of expertise: Arjun, Angad, Vidya, Raghu, and Pradeep. The plan for the complete week of prototyping was very structured with strict deadlines. We had numerous brainstorming sessions, we had to finalize the electronics, and we looked at form-factor. I also was fortunate to connect with Tata Fellows Anshuman Das and Guy Satat from the Camera Culture Group as well as many other passionate and dynamic researchers from MIT. I also met John Werner, the groups Head of Innovation. He is the liveliest and most inspiring person I have ever met, always with his camera, capturing every moment of the workshop.
The team from MIT, Ramesh, Anshuman, Guy, Rohan and Maulik, were instrumental in identifying mECG as one of the potential projects that could transform healthcare in India and developing countries. Year after year, healthcare workers in India work with thousands of patients in slum or rural communities who refuse to come to the hospitals for diagnostics. This can be because of the distance, inconvenience, or due to the cost of the visits. mECG is a direct response to these doctors’ call for help. It will enable them to aid the over six million slum inhabitants in Mumbai (half of this city’s overall population), and provides a tool to help rural communities throughout India.
At the end of this one week workshop we had a complete working prototype ready; a belt which can be worn on the chest to capture your single lead ECG and send it to a smartphone reliably using Bluetooth connectivity. It was a dream-come true when Mr. Ratan Tata visited each of the teams to see our demos. We received a strong support and collaboration from the Tata Center. I received positive feedback from various instructors and visitors and I was determined to work even more on this prototype to make sure that it would reach the hands of the needy.
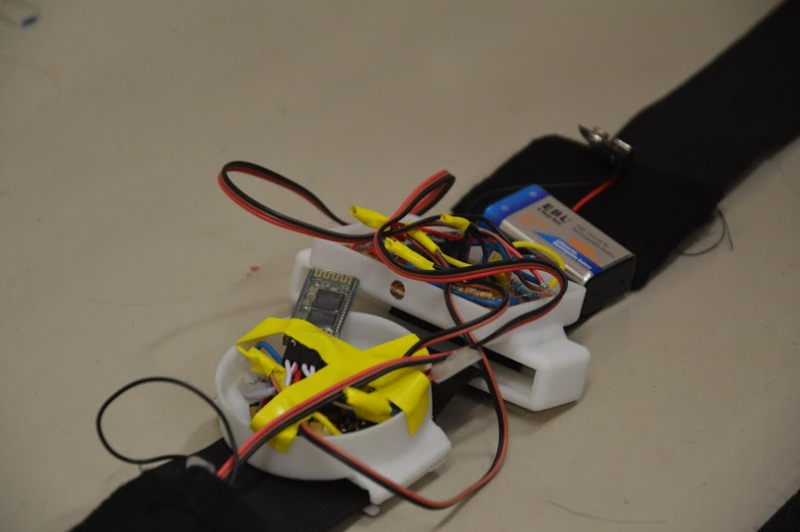

| Here are some snapshots of our first prototype which we built during the one week camp. Close-up of wearable ECG prototype developed at the MIT Health Tech workshop (left). Testing the prototype on one of the participants (right). |
After the workshop we started planning our path. We were determined to create an impact with our device and save millions of lives. All team members were in different locations, so we decided to divide our work and have weekly Google hangout’s to update one another. After brainstorming and seeking feedback from doctors, we decided on a few unique features to make our device unique. These features are: long-term continuous monitoring, wearable, dry electrodes and automated diagnosis in addition to it being low-cost.
I started working on algorithms which could filter the raw ECG data and accurately detect the P, QRS and T components in the ECG signal. By early May 2014, we had algorithms to detect Heart Rate (HR), Respiration Rate (RR) and accurately identify P, QRS and T complexes in the ECG signal. Arjun was ready with the ‘mECG’ Android App which could display the ECG signal in real-time and accurately calculate and display the HR, RR and detect if there is any irregularity.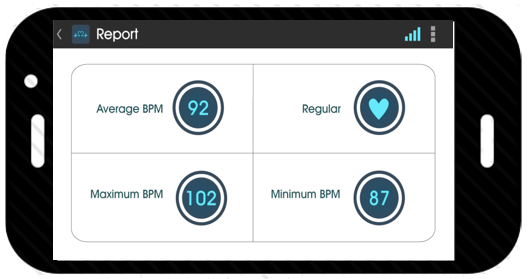
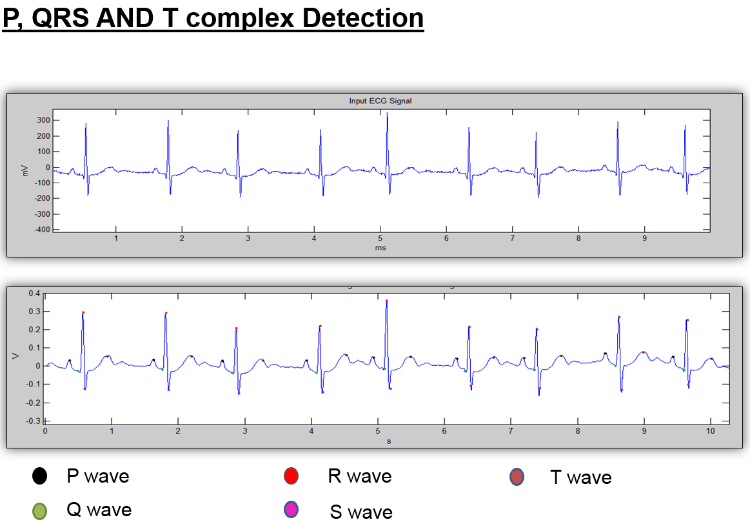
Snapshots of the App and the algorithm.
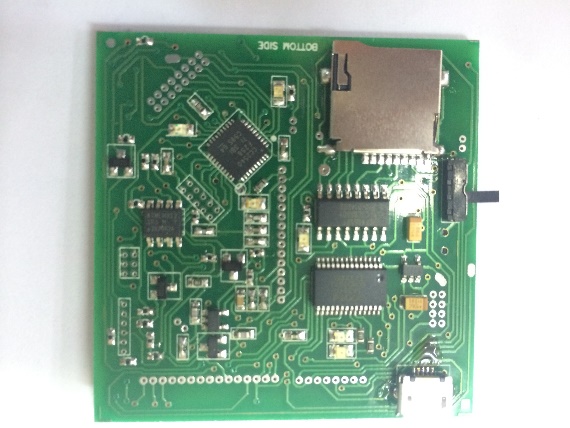
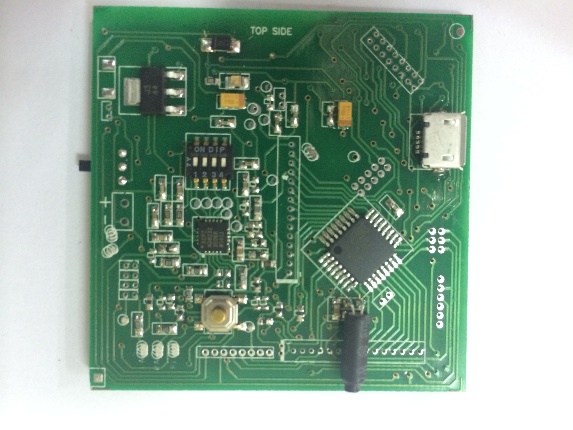
The key constrain was to design a low-power ECG amplifier which can continuously monitor ECG for at least 20 days without needing to charge the battery. We came up with a circuit, with ECG amplifier, controller, Bluetooth and SD card all embedded into a single PCB.
We all met again in June at IIT Bombay for the moth-long MIT Health Tech Internship. Our main goal was to carry out as many clinical trials in collarboaating hospitals in Mumbai to test our algorithm and understand the exact clinical needs. This would help us modify our device. We visited Hinduja and Holy Spirit Family Hospital to carry out the trials. This was the most tedious phase during the entire development cycle. It would take an entire day in the hospital to complete trials on just four to five patients with arrhythmias. Eventually we were able to get the ECG data from 10 patients suffering from Atrial Fibrillation. Our algorithm worked as expected. This internship was very fun. I really appreciate the effort of Anshuman Das, Rohan Puri, Thanasi Athanassiadis and Guy Satt. They managed the internship efficiently and it was successful.
After the internship I relocated to Singapore for my doctoral studies and Arjun moved to California. We were co-leaders of the project and we were in completely different locations. This created complicatins managing the project. To manage our time and work efficiently, we had to cut down the team. This was the most painful thing what I had ever done. By August, we finalized the core team of mECG: Rohan, Arjun, Maulik and I. Our targets were straight, we wanted our device to be in hands of needy ASAP!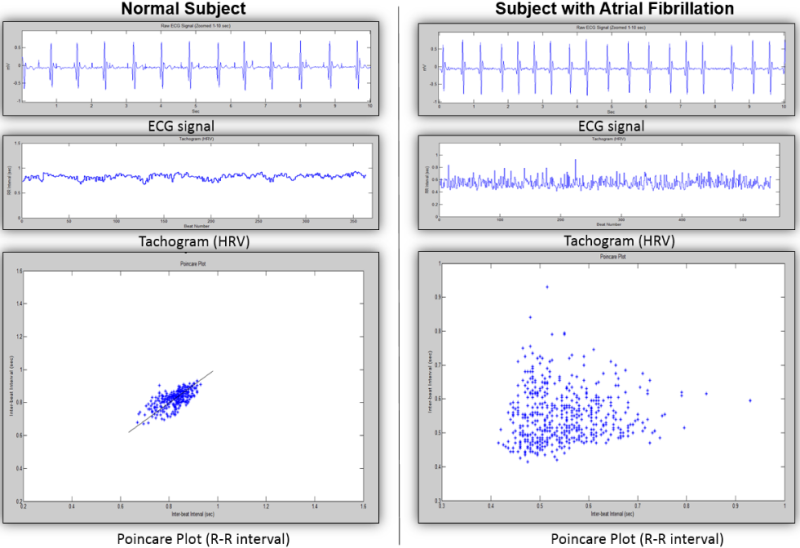
We then started working around the clock. When Rohan and Arjun slept in United States, I would work here in Singapore and vice versa. We were able to manage our time and make good progress in spite of being in different places. From August to December 2014 we went through three iterations of the circuit design and carried out a feedback survey from various cardiologists in India and China to study the market requirements. The response was amazing!
The following table gives you a complete summary of the whole development life cycle of ‘mECG’.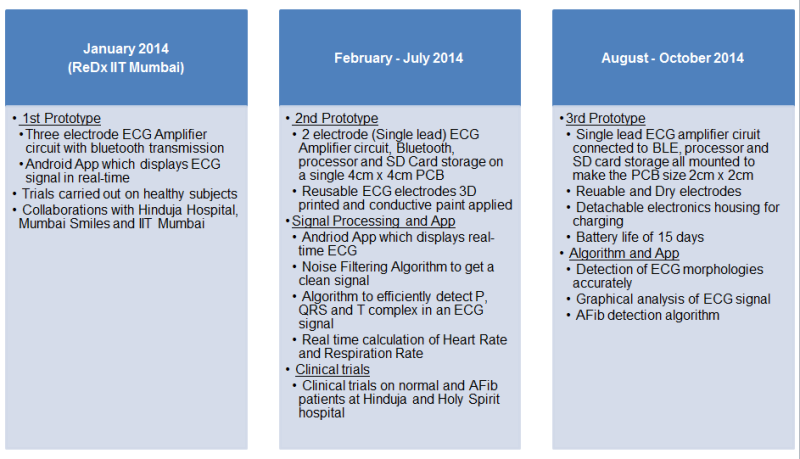
We are now working with PCB manufacturers and industrial designers in China and India to get our first set of 20-30 belts manufactured for pilot study and medical approval in India. We expect to have the devices ready by the end of January 2015. The final belt design and the key-features of the belt are shown below.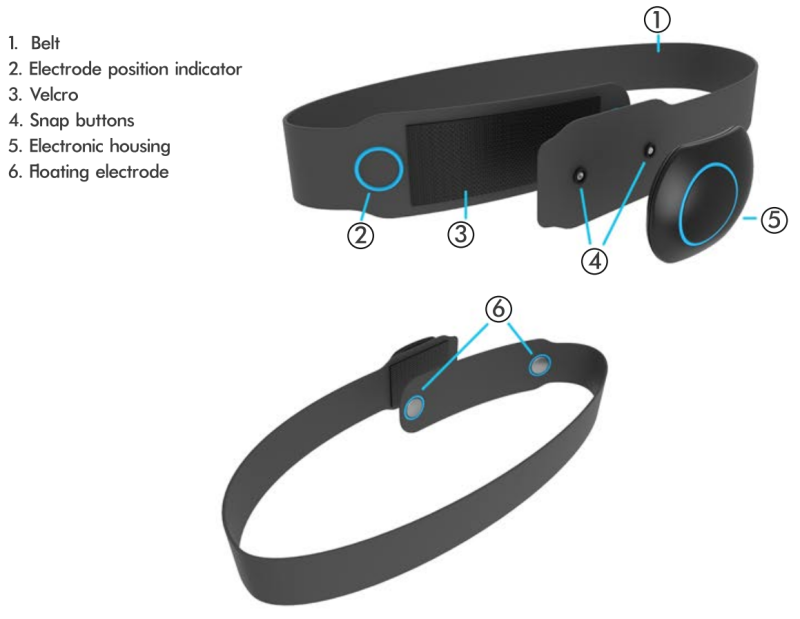
Key Features:
- Water-proof
- Dry-electrodes
- Detachable electronic housing with charging facility
- Sweat absorbent belt material
- Electrode contact check facility
- 20 days battery life
- Gender independent
- Low cost
Why mECG for India and Developing Countries:
In India, it is estimated that 32 million adults suffer from cardiovascular disease (CVD), representing one in three adult fatalities as per the extrapolation of Global Disease Burden Study. To put this number in perspective, it is almost equal to the population of Canada. It is a huge challenge that lies in front of India, with a significant growth in Non Communicable Diseases (NCD) and especially Cardio Vascular Diseases.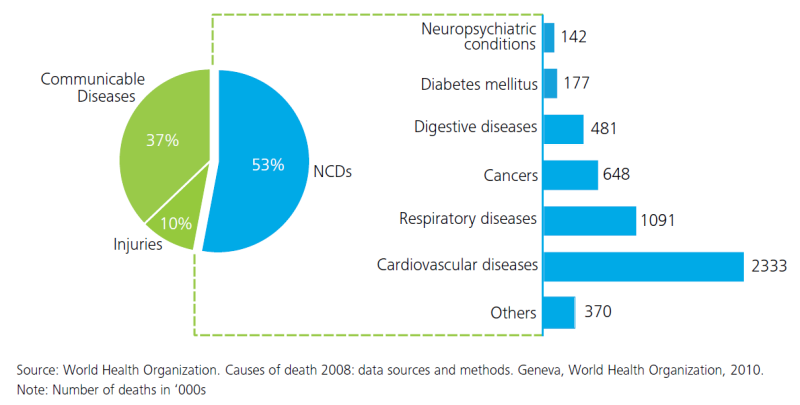
Between 2011 and 2031 it is estimated that the number of people above 60 years of age is expected to double. In rural areas, the symptoms of CVDs are ignored in the initial phases due to lack of diagnostic tools. They rush to the hospital in the last moment in case of a stroke by which time the disease has progressed to advance stage. Despite being a highly treatable disease, CVD continues to afflict populations largely due to lack of readily available, low-cost diagnostics. Hypertension is a major risk factor for CVD, but it often remains undiagnosed or untreated. Diagnostics such as regular blood pressure measurements and electrocardiograms can accurately identify at-risk hypertensive patients, and serve as the basis to decide on treatment options. However diagnostic tools remain inaccessible to large portions of the population. These tools are typically expensive, uncomfortable, and time consuming to use. They require a specialist to operate, and regular measurements to be most meaningful. Such circumstances disadvantage poor and rural communities in India from participating in preventative measures to curb CVD. If affordable and user-friendly diagnostic devices were available to these disadvantaged populations, CVD risk factors could be earlier identified, treated, and could be drastically reduced.
‘mECG’ is a unique device capable of tracking a patient’s electrocardiogram (ECG) in a non-intrusive and physician-friendly manner. Designed for usability and robustness, our devices not only allows for episodic ECG measurements, but can also be used for continuous (Holter) monitoring at a considerably lower cost. The data collected is automatically analysed to identify meaningful diagnostic features to better inform clinical decisions.
Outreach:
Our work was recognized by various healthcare associations, TEDx communities, and non-profit organizations. I was fortunate to be invited to speak and demonstrate the idea of mECG at one of the biggest TEDx event in India, TEDxTughlaqRd. It was a wonderful experience sharing the idea of mECG and how MIT Health Tech initiative has played a crucial role on our lives in this whole journey. Here is the link of my talk titled “Saving lives one phone at a time”
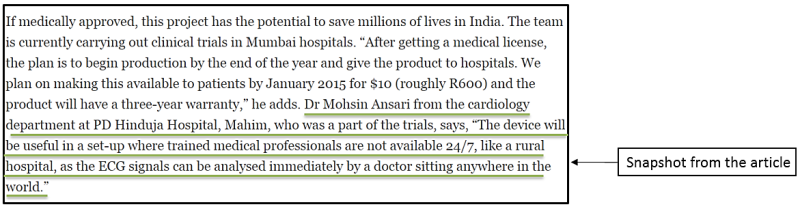
Immediately after my TEDx talk, we started getting requests for collaboration. HealthKart, one of the leading online shopping for healthcare products in India, extended their support and willingness to help us market the device. Also, we were recognized by the media. We were featured in Mid-Day Newspaper (July 2014) as one of the potential device which could save millions of lives in India. Here’s the link of the article.
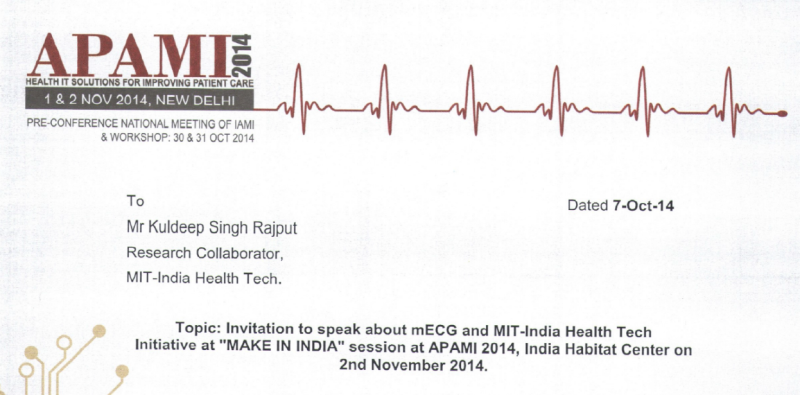
 In October I met Mr Rajendra Gupta, a versatile leader recognized for his contribution in diverse fields including public policy, governance reforms, innovation, healthcare, retail & rural economy. He is recognized as one of the top thinkers in the world, and he is among the most influential people in Soon, I was invited to speak at the “Make in India” session at 8th Asia Pacific regional meeting of International Medical Informatics Association. The conference attracted high profile doctors from AIIMS, members of WHO and IMIA. AIIMS will help us carry out the pilot study on various cardiovascular patients.
In October I met Mr Rajendra Gupta, a versatile leader recognized for his contribution in diverse fields including public policy, governance reforms, innovation, healthcare, retail & rural economy. He is recognized as one of the top thinkers in the world, and he is among the most influential people in Soon, I was invited to speak at the “Make in India” session at 8th Asia Pacific regional meeting of International Medical Informatics Association. The conference attracted high profile doctors from AIIMS, members of WHO and IMIA. AIIMS will help us carry out the pilot study on various cardiovascular patients.
Some highlights:
- We were invited to demonstrate ‘mECG’ at CAMTech India Clinical Summit 2014, Bangalore.
- We are the finalist at USC iStart Business-Tech competition 2014-15. Received a grant of $2.5K for preparation for the finals in March 2015. (http://mepc2015.istart.org/)
- mECG was quoted as an example for outstanding innovation at International Innovation Sustainability Entrepreneurship Summit 2014 (http://www.slideshare.net/rajendrapgupta/international-innovation-sustainability-entrepreneurship-summit-2014-iit-delhi)
The MIT Health Tech Workshop was very unique. It brought together students from across India to work closely with clinicians over seven days to develop fully functional prototypes for medical diagnostics, which went through rigorous design and evaluation followed by clinical testing in Mumbai hospitals. With MIT’s deep expertise in health and wellness technologies, the goal of the workshop was to provide an open innovation platform for students and researchers. The designed prototypes were explored well beyond the workshop, with serious mentoring, funding and working space. I feel fortunate to be a part of this workshop and the whole journey.
When I was young, I had many ideas and working prototypes, but I was never successful bringing these to the market. Getting a device, especially a medical device, to market involves a completely different trajectory of innovation and development life cycle. This requires constant support, motivation and most importantly opportunities. The MIT Health Tech Initiative has been instrumental in providing me with these opportunities and constant support to transform me into a tech-minded entrepreneur. I have learned to be leader, fight challenges in the product development stage, manage a team efficiently, and negotiate with investors in just one year.
I am confident that ‘mECG’, the first medical device to be commercialized from the MIT Health Tech Initiative, will create a significant impact and benefit to those in need. The device will transform the process of cardiac care in India.
Journey of ‘mECG’ over the last 11 months
Stages of development:
Team mECG at MIT Health Tech workshop: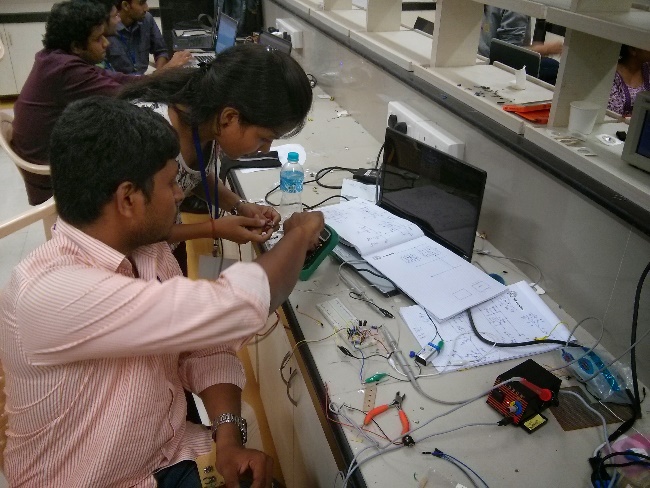


 The MIT Team and Clinicians with Mr. Ratan Tata and Dr. Ramesh Raskar
The MIT Team and Clinicians with Mr. Ratan Tata and Dr. Ramesh Raskar At MIT Health Tech Internship (Posing with the future glasses) with Rohan Puri and Dr. Maulik Majmudar
At MIT Health Tech Internship (Posing with the future glasses) with Rohan Puri and Dr. Maulik Majmudar
Demonstrating ‘mECG’ live, on an attendee at the TEDx event during my talk
To know more about mECG, visit the website www.mekg.in
Instructor at Kumbhthon:
The Kumbh Mela is one of the largest festivals in the world which draws around 10 million pilgrimages across the world.
KumbhaThon is a technical buildathon for Kumbh 2015. It is a weeklong ideating and prototyping extravaganza. Participants develop, prototype and deploy innovative solutions to the issues faced by the pilgrims, like healthcare, crowd-management, sanitation, safety etc. I was invited to the event as an Instructor by Prof. Ramesh Raskar, who was also born in Nashik and had a vision to solve the issues faced by the event attendees using technology and innovation.
It was an amazing experience at Nashik meeting some passionate local leaders like Sunil Khandbahale. I also met some fantastic fellow mentors, Vijay Sadashivaiah, Nilesh Nayak and Vaibhav Chabra. I was mentoring few projects in the ‘crowd management’ vertical. We used 3D printers to prototype the devices quickly and get then working. We had several rounds of brainstorming sessions before we finalized the design and then started implementing.
I personally feel that Nashik has the potential to generate more potential innovators and leaders like Ramesh and Sunil. I will also be joining the next edition of the event which is happening in the month of January 2015.
Learn more about this initiative: http://kumbha.org
Instructors with Prof. Ramesh
Prof. Ramesh presenting Kumbahthon initiative at INK 2014

About me: I am Kuldeep Singh Rajput, a PhD research scholar at National University of Singapore (NUS). My research mainly focuses on neuro-devices, massive neural stimulation, recording and data analysis. My principal fields of interest are Wearable medical devices, neural data analysis, Analog design, Medical Imaging and Human Computer Interfaces.
I spent my childhood in a small town called Belgaum in South India. I finished my matriculation from The Forbes Academy and then joint GSS Pre University College. I completed my undergrad degree in the year 2013 from Visvesvaraya Technological University with major in Electrical and Electronics Engineering. I am the winner of ‘Young Innovator Award’ of India, granted by Department of Science and Technology, Government of India and Confederation of Indian Industries (CII). I have always been an active member in the events conducted by MIT Media Lab. I have been a part of ReDx initiative as well as Kumbhathon, Nashik.
I aspire to build neural-technologies which systematically map the brain and computations that it performs. I focus on pushing out working prototypes and closing the gap between engineering and medicine.
